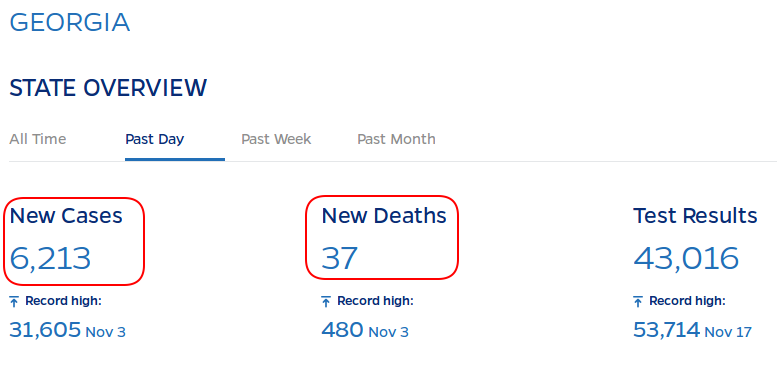
I could talk about the Georgia run-offs, but that’s pretty much as I expected: Dominion scanners selectively not working in Republican strongholds, observers blocked from viewing the process, dubious ballot adjudication by unsupervised/observed individuals, Democrat strongholds stopping the count in the middle of the night…
Same people with the same systems breaking the same laws.
But let’s talk about something else. ChinCOVID, COVID-19, SARS-CoV-2.
Start with this paper. Be warned it’s technical.
External peer review of the RTPCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false positive results.
This paper will show numerous serious flaws in the Corman-Drosten (C-D) paper, the significance of which has led to worldwide misdiagnosis of infections attributed to SARS-CoV-2 and associated with the disease COVID-19. We are confronted with stringent lockdowns which have destroyed many people’s lives and livelihoods, limited access to education and these imposed restrictions by governments around the world are a direct attack on people’s basic rights and their personal freedoms, resulting in collateral damage for entire economies on a global scale.
TL;DR: The Corman-Drosten paper being criticized is the basis of the RNA PCR test for ChinCOVID. And it’s BS.
I was very much aware of one major problem with the PCR test: a very high amplification cycle rate. The more you amplify, the more “noise” you amplify. More than 30 cycles is unusual for a PCR test. Specific research into the number of cycles for ChinCOVID has shown that samples that test positive at more than 30 cycles has no more than a 50:50 chance of being real. That is, a swab that tests positive at 30 cycles has a 50:50 chance of being successfully cultured. That’s even odds of a viable virus being present.
At 35 cycles 97% of the samples cannot be successfully cultured; there was no viable virus present.
The CDC recommends 40+ cycles.
That’s the problem I knew about. But read this paper, and you’ll see it’s fatally flawed.
The C-D test examines two genes for specific nucleotide combinations, allegedly specific to ChinCOVID. But the test was designed without access to an actual SARS-CoV-2 virus, live or otherwise. C-D assumed that it was the same family as the old SARS-CoV, and looks for one sequence from that. Then it looks for a second sequence that was published by the Chinese in a public database, which came from SARS-CoV-2.
But… there is a third gene, with a nucleotide sequence that has only been found in two beta-corona viruses: SARS-C0V and SARS-CoV-2. It’s perfect for excluding other betacoroanviruses, making the test definitively specific for SARS-CoV-2.
The ChinCOVID PCR test does not check for that specific third gene.
Turns out there are other problems with the described test protocol… as in the protocol isn’t really specified. Temperatures for reactions at different stages of the test aren’t specified. That will affect the accuracy. It doesn’t specify the number of amplification cycles.
Even C-D admitted their test generated a high number of false positives. They’d get a positive on a sample, retest it multiple times and keep getting negatives.
The C-D PCR test is bullshit. It will pop positive for most betacoronaviruses.
Interestingly, back in April — when everyone was scrambling for tests — a Florida researcher repurposed an old test for ChinCOVID. Dr. Lednicky very kindly took time away from his work to describe his test to me (because the “news” reporter so botched the description of it that I thought it was impossible for it to work). Dr. Lednicky described how he modified his existing test to look for the ChinCOVID-specific nucleotide sequence. And he mentioned that his previous test (it was designed to find new, unknown viral variants in the field) had a factor that excluded other known human betacoronaviruses.
Now that I know about the C-D test flaw, I’d bet that Dr. Lednicky’s “exclusion factor” is that very third gene that C-D doesn’t bother checking.
| If you found this post useful, please consider dropping something in my tip jar. I could really use the money, what with ISP bills, rabbit feed, and general life expenses.Click here to donate via PayPal. |